
Research - International Journal of Medical Research & Health Sciences ( 2023) Volume 12, Issue 1
Effect of Foot Reflexology on Vital Parameters and Anxiety of Hypertensive Patients: A Clinical Trial Study
Zahra Najafiana1* and Mahmood Najafian22Endocrinology and Metabolism Research Center, Tehran University of Medical Sciences, Tehran, Iran
Zahra Najafiana, School of Nursing and Midwifery, Shiraz University of Medical Sciences, Shiraz, Iran, Email: zahranajafian@sums.ac.ir
Received: 12-Dec-2022, Manuscript No. ijmrhs-22-83168; Editor assigned: 14-Dec-2022, Pre QC No. ijmrhs-22-83168(PQ); Reviewed: 24-Dec-2022, QC No. ijmrhs-22-83168(Q); Revised: 29-Dec-2022, Manuscript No. ijmrhs-22-83168(R); Published: 20-Jan-2023
Abstract
Introduction: Complementary medicine interventions are now successfully used to stabilize physiological parameters and reduce anxiety within different procedures. The present study aimed to examine the effect of foot reflexology on stabilization physiological parameters and reducing anxiety in hypertensive patients. Methods: In this clinical trial, 90 hypertensive patients were assigned to intervention (received foot reflexology), placebo (received general foot massage), and control (received only routine care of the hospital) groups. Anxiety levels and vital signs were measured before, immediately after, and half an hour after the intervention. Results: Based on our findings in this study, systolic blood pressure, heart rate, and respiratory rate in the intervention and placebo groups were significantly reduced compared to the control group. Diastolic blood pressure and level of oxygen saturation showed a significant decrease only in the intervention group compared to the control group. The findings of this study also showed that the level of state and trial anxiety in the intervention and placebo groups was significantly lower than in the control groups. Conclusion: The results of this study and most of the research done, show that foot reflexology has a positive effect on improving physiological factors and anxiety in hypertensive patients. Therefore, foot reflexology as a method of complementary medicine in these patients can be useful and effective.
Keywords
Reflexology, Hypertension, Vital parameters, Anxiety
Introduction
High blood pressure affects 30% of adults and is the most important risk factor for heart attack and stroke. Hypertension is thought to be a disorder of the two systems involved in regulating water-salt balance and cardiovascular function. High blood pressure is a major cause of global mortality and is also a major symptom of cardiovascular disease [1-3]. Hypertensive is a term referring to high Blood Pressure (BP) and BP does not remain at the same level all the time. Furthermore, it is defined as a persistent elevation of the Systolic Blood Pressure (SBP) at a level of 140 mm Hg or higher and Diastolic Blood Pressure (DBP) at a level of 90 mm Hg or higher. Some hypertensive patients may have a headache, dyspnea, and epistaxis [4-7]. The prevalence of high blood pressure in obese people is 2 times to 3 times higher than in non-obese people. Obesity at an early age is an important factor in increasing blood pressure in adulthood. Along with this obesity, the sympathetic nervous system, hypersensitivity to sodium/salt retention, and insulin resistance are implicated in causing high blood pressure. In addition to the above, sleep apnea syndrome, which is common in these patients, may be another factor in causing high blood pressure [5,8]. Today, the world is facing an outbreak of an epidemic caused by the acute respiratory syndrome of coronavirus SARS-CoV-2, which causes a disease called COVID-19. The most common comorbidities are hypertension (30%), diabetes (19%), and cardiovascular disease (8%) [9-10]. The prevalence of hypertension is associated with age, mental stress, and anxiety. Stress and anxiety are the main causes of high blood pressure [11]. Dyslipidemia is another complication of hypertension that is associated with abnormal lipid metabolism [5]. Numerous studies have shown that there is a direct relationship between dietary sodium intake and blood pressure [12, 13]. The incidence of hypertension is attributed to a disorder of two systems that are involved in the regulation of saltwater balance and cardiovascular function, namely the renin-angiotensin-aldosterone system and the sympathetic nervous system [1]. Some endocrine disorders can cause high blood pressure. Hypo and hyperthyroidism, elevated levels of anti-Natriuretic hormones such as angiotensin II, aldosterone, and adipokines, especially leptin, can cause high blood pressure [8,12]. Hypertension is treated with both pharmacological and non-pharmacological methods. Medication includes the use of Diuretics, AngiotensinConverting Enzyme (ACE) inhibitors, Aldosterone inhibitors, Beta blockers, Renin inhibitors, Peripheral alphablockers, Centrally-acting alpha- 2 agonists, and direct vasodilators [6]. In the non-pharmacological control and treatment of hypertension, most physicians recommend that lifestyle changes and complementary medicine be used for treatment before prescribing drugs [14]. Complementary and alternative medicine includes various methods of treatment and prevention of diseases, the method and effectiveness of which is different from conventional and biological medicine and includes a set of practices and ideas used by patients to prevent and treat diseases or improve health and improve the general condition of the patient is used in conjunction with conventional therapies. These treatment methods include acupuncture, herbal remedies, dietary supplements, aromatherapy, yoga, massage therapy, reflexology, and several others [15]. Foot reflexology is one of the complementary therapy. Foot reflexology has mechanical effects that improve circulation, remove waste products from the body, improve joint mobility, relieve pain and reduce muscle tension [16,17]. Foot reflexology is a systematic practice in which applying some pressure to any particular point on the feet give impacts the health of related parts of the body. In reflexology, it is believed that the legs are a small map of the whole body and that the specific reflex stimulation at each point on the sole corresponds to the corresponding part of the body [18-21]. Nowadays people tend to use non-drug methods and alternative medicine for reducing the effects of drug side effects. Because the prevalence of hypertension is high, especially in adults and there are contradictory results on the effect of reflexology on hypertension. This study aims to investigate the effect of foot reflexology on physiological parameters and anxiety of hypertensive patients.
Methods
Design
This study was a three-group single-blind randomized clinical trial. This study was approved by the Ethics Committee of Shiraz University of Medical Sciences (IR.SUMS.REC.1399.1278, approval date: 2021-04-03). Consent forms were signed by all participants. They were informed that participation in the study was voluntary and that they could stop at any time.
Sample size and Participants
Using a pilot study and based on power=80%, α=0.05, mean scores of Systolic Blood Pressure (SBP) in the intervention, placebo, and control groups=144.3, 156.6 and 160.2 mmHg respectively, and standard deviation=18.7. Moreover, using that pilot study and considering power=80%, α=0.05, mean scores of anxiety in the intervention, placebo, and control groups=55.2, 60.4, and 62.5 respectively, and standard deviation=8.3. Based on the following sampling formula:
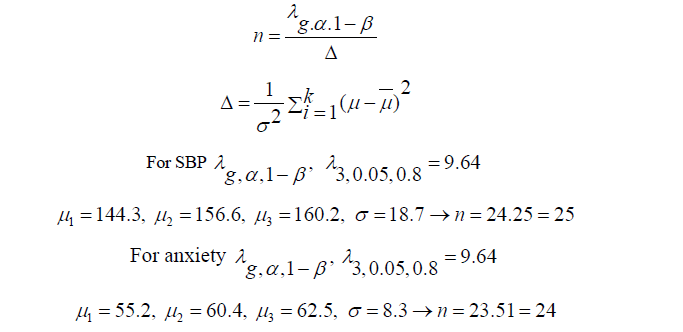
Therefore, the highest sample size in each group was 25 (75 patients in total). Based on a dropout rate of 20%, the sample size was raised to 90 (30 patients in each group). During the study, none of the patients dropped out and all 90 patients finished the study (Figure 1).

Figure 1.The process of the study, according to the Consort flow chart
The subjects of this study consisted of 90 eligible hypertensive patients. The study was conducted in Coronary Care Units at Al-Zahra Heart Centre affiliated with Shiraz University of Medical Sciences, Shiraz, Iran. Patients were randomly allocated and divided into equal numbers, to 30 patients in the intervention, placebo, and control groups.
Inclusion and Exclusion Criteria
Subjects were eligible for inclusion in the study if they were: Adult males and females, aged 41 years to 70 years, had hypertension (systolic blood pressure greater than or equal to 140 mmHg, and diastolic blood pressure greater than or equal to 90 mmHg), have not taken antihypertensive and anti-anxiety drugs 48 hours before the intervention, speak Persian language and oriented to time, person and place. Subjects were excluded from the study if they had an infectious or bleeding ulcer in their legs, had undergone foot surgery, inability to tolerate foot reflexology massage, were pregnant women, had recent major surgery such as open heart surgery, had diabetic foot complications, and had irregular heart rate.
Measures
Data were collected using two questionnaires and a digital heart monitoring device. The first questionnaire contained items on participants' demographic characteristics, including age, gender, BMI, marital status, smoking, and history of hypertension and diabetes. The second questionnaire was Spielberger's State-Trait Anxiety Inventory (STAI) a self-administered questionnaire. The score of the inventory could range from 20 to 80, with higher scores representing greater anxiety [22]. Monitors were used to measuring Systolic Blood Pressure (SBP), Diastolic blood pressure (DBP), Heart Rate (HR), and Respiratory Rate (RR). Also, O2 saturation (SPO2) was measured using a pulse oximetry device. The outcomes of this study were anxiety levels and vital parameters that were measured before, immediately after, and half an hour after the intervention. According to research by John et al. The shortterm and immediate effects of massage therapy occur 20 minutes to 30 minutes after massage therapy [23].
Intervention
All the interventions in three groups were performed by a certified reflexologist (the first author) on the morning shift. Room conditions, including the amount of light, traffic, and noise, the three groups were almost identical. Before starting the procedure, anxiety levels and vital parameters were measured. In the intervention group, reflexology was done for each patient for 30 minutes (15 minutes for each foot) [24,25]. In the reflexology group, the patient was assisted to lie down in a supine position by raising the head of the bed to 30 degrees. To do reflexology, firstly the reflexologist washed his hands with warm water and rubbed them together to warm them. Secondly, she warmed the patient's foot rubbing it with his hands using sweet almond oil to facilitate massaging [25]. When the foot was sufficiently warm and received relaxation and general foot massage, four major plantar reflexology points (solar plexus, pituitary gland, heart, and liver) were put under pressure using the thumbs [20-27]. The reflexologist applied downward pressure with her thumb in each area for two minutes. The pressure was adjusted to whiten the pressure on the thumb in the area, but the patients did not feel any pain. A rotational massage was then applied to specific areas [26,27]. The placebo group received a general foot massage without stimulating the reflexology points [27]. The control group did not receive any type of massage. It should be noted that all three groups were under the usual care of the hospital.
Statistical Analyses
Data were analyzed by SPSS software version 23. Descriptive statistics including numbers and percentages were used for qualitative variables, and the mean and standard deviation for quantitative variables. The chi-Square test was used to assess the similarity between the three groups in terms of demographic characteristics. The repeated measures of analysis of variance (RM-ANOVA) test was used to compare anxiety levels and physiological parameters in each group across the three measurement time points. The one-way analysis of variance (ANOVA) test and Tukey's post hoc test were also used for comparing the groups in terms of anxiety levels and physiological parameters at each measurement time point. The statistical significance level p-value was set at less than 0.05.
Results
Demographic Characteristics
In total, 90 patients were recruited for the study, all of whom remained in the study until its end (Figure 1). Based on Table 1, most patients were over 55 years old. The majority of the patients in all groups were male and married. Most patients had a BMI equal to or less than 30 (Kg/m2 ). About half of them had a history of more than five years of high blood pressure. The results showed that 13.3% of the participants had diabetes and 16.6% of the patients were smokers. According to Table 1, the results showed that the three groups were homogenous concerning demographic and clinical characteristics.
| Variables | Intervention N (%) | Placebo N (%) | Control N (%) | Chi-square test |
|---|---|---|---|---|
| Age | ||||
| 41 years-55 years | 10(33.3%) | 12(40.0%) | 9(30.0%) | X2=0.689 |
| 56 years-70 years | 20(66.6%) | 18(60.0%) | 21(70.0%) | p=0.709 |
| Gender | ||||
| 22(73.3%) | 23(76.6%) | 21(70.0%) | X2=0.341 | |
| Female | 8(26.6%) | 7(23.3%) | 9(30.0%) | p=0.843 |
| BMI(Kg/m2) | ||||
| BMI ≤ 30 | 24(80.0%) | 26(86.6%) | 27(90.0%) | X2=1.259 |
| BMI>30 | 6(20.0%) | 4(13.3%) | 3(10.0%) | p=0.533 |
| Marital status | ||||
| Single | 6(20.0%) | 8(26.6%) | 5(16.6%) | X2=0.934 |
| Married | 24(80.0%) | 22(73.3%) | 25(83.3%) | p=0.627 |
| Smoking | ||||
| yes | 6(20.0%) | 4(13.3%) | 5(16.6%) | X2=0.480 |
| No | 24(80.0%) | 26(86.6%) | 25(83.3%) | p=0.787 |
| History of Hypertension | ||||
| ≤ 5 years | 18(60.0%) | 15(50.0%) | 16(53.3%) | X2=0.627 |
| >5 years | 12(40.0%) | 15(50.0%) | 14(46.6%) | p=0.731 |
| Diabetes | ||||
| Yes | 4(13.3%) | 3(10.0%) | 4(13.3%) | X2=0.207 |
| No | 26(86.6%) | 27(90.0%) | 26(86.6%) | p=0.902 |
Vital Signs
Table 2 compares the vital signs between the study groups. The results of the one-way ANOVA illustrated that at baseline, there was no significant difference among the groups regarding the level of vital signs (p>0.05). The results of Repeated Measures Analysis Of Variance (RM-ANOVA) showed that some factors in the intervention and placebo groups immediately and half an hour after the intervention had significant changes. According to Table 2 and Figure 2, the amount of SBP in the intervention and placebo groups decreased significantly during these three measured points (p˂0.001). Based on Table 2, the DBP showed a significant decrease only in the intervention group (p˂0.01). There was a significant decrease in HR in the intervention group (p˂0.001) and in the placebo group (p=0.002) across the three measurement time points. A statistically significant reduction in the RR was noted (p=0.006) and (p=0.025) in the intervention and Placebo groups, respectively. The percentage of oxygen saturation was significantly increased only in the intervention group in the three measurement time points (p=0.027).
| Variables Groups |
Before the Intervention | Immediately after the Intervention |
Half an Hour after the Intervention |
RM-ANOVA |
|---|---|---|---|---|
| Systolic blood pressure | ||||
| >Intervention | 154.40 ± 12.35 | 154.17 ± 12.37 | 153.87 ± 12.26 | F=19.50, p˂0.001 |
| >Placebo | 154.53 ± 12.28 | 154.37 ± 12.33 | 154.13 ± 12.36 | F=12.59, p˂0.001 |
| >Control | 154.60 ± 12.35 | 154.57 ± 12.35 | 154.53 ± 12.28 | F=1.53, p=0.23 |
| >ANOVA | F=0.002, p=0.99 | F=0.008, p=0.99 | F=0.022, p=0.98 | |
| Diastolic blood pressure | ||||
| >Intervention | 101.73 ± 9.23 | 101.63 ± 9.11 | 101.53 ± 8.93 | F=5.12, p˂0.01 |
| >Placebo | 102.70 ± 9.53 | 102.57 ± 9.27 | 102.50 ± 9.14 | F=3.83, p=0.06 |
| >Control | 104.00 ± 9.36 | 104.03 ± 9.48 | 103.97 ± 9.46 | F=1.53, p=0.23 |
| >ANOVA | F=0.44, p=0.64 | F=0.51, p=0.60 | F=0.53, p=0.59 | > |
| Heart rate | ||||
| >Intervention | 79.63 ± 6.37 | 79.43 ± 6.36 | 79.20 ± 6.53 | F=14.00, p˂0.001 |
| >Placebo | 80.20 ± 6.33 | 80.07 ± 6.33 | 79.93 ± 6.45 | F=7.25, p=0.002 |
| >Control | 80.23 ± 6.32 | 80.17 ± 6.31 | 80.13 ± 6.31 | F=2.45, p=0.110 |
| >ANOVA | F=0.08, p=0.92 | F=0.12, p=0.89 | F=0.17, p=0.84 | |
| Respiratory rat | ||||
| >Intervention | 14.97 ± 1.73 | 14.90 ± 1.64 | 14.73 ± 1.57 | F=6.61, p=0.006 |
| >Placebo | 15.43 ± 1.77 | 15.40 ± 1.77 | 15.27 ± 1.64 | F=4.72, p=0.025 |
| >Control | 15.20 ± 1.69 | 15.13 ± 1.59 | 15.10 ± 1.58 | F=2.45, p=0.110 |
| >ANOVA | F=0.54, p=0.58 | F=0.67, p=0.51 | F=0.87, p=0.42 | |
| O2 Saturation | ||||
| >Intervention | 95.37 ± 1.37 | 95.43 ± 1.38 | 95.53 ± 1.31 | F=4.21, p=0.027 |
| >Placebo | 95.50 ± 1.33 | 95.53 ± 1.31 | 95.60 ± 1.33 | F=2.45, p=0.110 |
| >Control | 95.43 ± 1.45 | 95.47 ± 1.48 | 95.50 ± 1.48 | F=1.53, p=0.229 |
| >ANOVA | F=0.07, p=0.93 | F=0.04, p=0.96 | F=0.4,p=0.96 | > |

Figure 2. Systolic blood pressure in intervention, placebo and control group
Anxiety Level
The results of the one-way ANOVA showed that, before the intervention, there was no significant difference among the groups regarding the level of State and trial anxiety. The results of the RM-ANOVA showed a statistically significant decrease in the state and trial anxiety (p˂0.001) in intervention and placebo groups across the three measurement time points (Table 3 and Figure 3).
| Variables Groups |
Before the Intervention |
Immediately after the Intervention |
Half an Hour after the Intervention |
RM-ANOVA |
|---|---|---|---|---|
| State anxiety | ||||
Intervention |
43.13 ± 9.85 | 41.83 ± 9.25 | 41.70 ± 9.10 | F=69.44, p˂0.001 |
Placebo |
43.43 ± 8.85 | 42.93 ± 8.56 | 42.80 ± 8.60 | F=29.19, p˂0.001 |
Control |
43.70 ± 9.11 | 43.63 ± 9.12 | 43.70 ± 9.10 | F=1.00, p=0.37 |
ANOVA |
F=0.02, p=0.97 | F=0.03, p=0.74 | F=0.38, p=0.69 |
|
| Trial anxiety | ||||
Intervention |
44.10 ± 9.68 | 42.70 ± 9.01 | 42.57 ± 9.05 | F=64.78, p˂0.001 |
Placebo |
44.33 ± 8.83 | 43.73 ± 9.09 | 43.60 ± 9.13 | F=30.02, p˂0.001 |
Control |
44.67 ± 9.11 | 44.60 ± 9.11 | 44.63 ± 9.11 | F=1.53, p=0.23 |
ANOVA |
F=0.03, p=0.97 | F=0.33, p=0.72 | F=0.39, p=0.68 |
|
| Total anxiety | ||||
Intervention |
87.23 ± 19.53 | 84.53 ± 18.24 | 84.17 ± 17.97 | F=79.08, p˂0.001 |
Placebo |
87.77 ± 17.68 | 86.67 ± 17.63 | 86.40 ± 17.72 | F=81.70, p˂0.001 |
Control |
88.37 ± 18.21 | 88.23 ± 18.22 | 88.33 ± 18.20 | F=2.26, p=0.12 |
ANOVA |
F=0.03, p=0.97 | F=0.32, p=0.73 | F=0.40, p=0.67 | |

Figure 3. Results of state anxiety level changes in intervention, placebo and control groups
Discussion
The effect of foot reflexology on vital parameters and anxiety of hypertensive patients was examined in this study. The results of this study showed that reflexology has beneficial and effective effects in hypertensive patients. RMANOVA showed that in the intervention and placebo groups, some factors had a significant change in these three measured points. The results of this research confirm the hypothesis that foot reflexology positively affects the stabilization of vital signs (SBP, DBP, HR, RR, and SPO2). This improvement can be based on the fact that there are about 15,000 nerves throughout the body in the feet. Therefore, using the reflexology method calms the nervous system and this improvement has occurred through this nervous relaxation [21]. According to the findings of this study, systolic blood pressure, heart rate, and respiratory rate were significantly reduced in the intervention and placebo groups during the three measured points. Diastolic blood pressure showed a significant decrease only in the intervention group, also the percentage of oxygen saturation increased significantly only in the intervention group. Our results are consistent with previous studies that have shown the effectiveness of the foot reflexology technique in improving physiological parameters [28-32]. A similar study has shown that reflexology has significantly improved physiological symptoms including SBP, DBP, HR, RR, and SPO2 in patients undergoing coronary angiography [26]. In this regard, our findings are consistent with other studies that have found evidence that foot reflexology reduces SBP and DBP [33]. A study reported that reflexology had a positive effect on reducing SBP and DBP but did not have a significant effect on HR and RR [20]. The inconsistency in the effects of the reflexology is related to factors such as reflexology performed by different individuals, the use of a small sample size, and changes in the number and duration of reflexology sessions [34-36]. Another factor that was examined in this study was the level of anxiety in these patients. The results showed that the level of the state, trial, and total anxiety in the intervention and placebo groups was significantly reduced during the three measured points. On the same line, our findings are consistent with other studies which obtained evidence that foot reflexology decreases state and trial anxiety [37-40]. Contrary to our findings, one study found that foot reflexology was ineffective in reducing anxiety among candidates for coronary artery bypass graft surgery [22]. This difference in results can be due to a variety of reasons, such as the size of the small sample, the use of anti-anxiety drugs, or participation in similar experiments [22]. The exact mechanism of action of reflexology in reducing anxiety is not yet known. Reflexologists believe that reflexology exerts its effects in reducing anxiety by stimulating the release of endorphins and enkephalins. These hormones lead to happiness and relaxation [22].
Conclusion
Hypertension affects one-third of adults and is the leading risk factor for heart attack and stroke, and premature death worldwide. The results of this study and most of the research show that foot reflexology has a positive effect on improving physiological factors and anxiety in patients with hypertension. In comparison, in all cases, the positive effects of reflexology in the intervention group were more than a general massage in the placebo group. Observations suggest that both types of massage can be beneficial in many cases, but reflexology is a more effective method. Therefore, foot reflexology as a method of complementary medicine in these patients can be useful and effective. However, extensive future studies are needed to provide strong evidence to support this approach and to enrich the knowledge base in this area.
Declarations
Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Acknowledgment
We thank all the patients who participated in this study and also all the staff of the departments of Coronary Care Units in Al-Zahra Heart Center affiliated with Shiraz University of Medical Sciences.
Financial Support
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Drummond, Grant R., et al. "Immune mechanisms of hypertension." Nature Reviews Immunology, Vol. 19, No. 8, 2019, pp. 517-32.
Google Scholar Crossref - Mills, Katherine T., Andrei Stefanescu, and Jiang He. "The global epidemiology of hypertension." Nature Reviews Nephrology, Vol. 16, No. 4, 2020, pp. 223-37.
Google Scholar Crossref - Song, Juan-Juan, et al. "Gender differences in hypertension." Journal of cardiovascular translational research, Vol. 13, No. 1, 2020, pp. 47-54.
Google Scholar - Ravindranath, BW., et al. ''Effect of foot reflexology on blood pressure & level of stress among hypertensive patients.'' Sinhgad College of Nursing, Vol. 7, No. 1, 2017, pp. 88-92.
- Umemura, Satoshi, et al. "The Japanese Society of Hypertension guidelines for the management of hypertension (JSH 2019)." Hypertension Research, Vol. 42, No. 9, 2019, pp. 1235-81.
Google Scholar Crossref - Leung, Alexander A., et al. "Hypertension Canada's 2017 guidelines for diagnosis, risk assessment, prevention, and treatment of hypertension in adults." Canadian Journal of Cardiology, Vol. 33, No. 5, 2017, pp. 557-76.
Google Scholar Crossref - Nerenberg, Kara A., et al. "Hypertension Canada’s 2018 guidelines for diagnosis, risk assessment, prevention, and treatment of hypertension in adults and children." Canadian Journal of Cardiology, Vol. 34, No. 5, 2018, pp. 506-25.
Google Scholar Crossref - Hall, John E., et al. "Obesity, kidney dysfunction and hypertension: mechanistic links." Nature reviews nephrology, Vol. 15, No. 6, 2019, pp. 367-85.
Google Scholar Crossref - Bosso, Mira, et al. "The two faces of ACE2: the role of ACE2 receptor and its polymorphisms in hypertension and COVID-19." Molecular Therapy-Methods & Clinical Development, Vol. 18, 2020, pp. 321-27.
Google Scholar Crossref - Fang, L., and G. Karakiulakis. "Roth MAre patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection." Lancet Respir Med, Vol. 8, 2020, p. e21.
Google Scholar Crossref - Missiriya, Sahbanathul, J. Suhail Hassan, and Arul Anunncia. "Effect of Reflex Therapy on Stress and Blood Pressure among Older Adults with Hypertension." Methodology, 2019.
Google Scholar Crossref - Berta, Eszter, et al. "Hypertension in thyroid disorders." Frontiers in endocrinology, Vol. 10, 2019, p. 482.
Google Scholar Crossref - Grillo, Andrea, et al. "Sodium intake and hypertension." Nutrients, Vol. 11, No. 9, 2019, p. 1970.
Google Scholar Crossref - Thomas, VA., et al. ''Effect of Foot Reflexology on Vital Parameters of Hypertensive Patients.'' Indian Journal of Nursing Studies, Vol. 7, No. 2, 2016, pp. 48-58.
- Grealish, Laurie, Angela Lomasney, and Barbara Whiteman. "Foot massage: a nursing intervention to modify the distressing symptoms of pain and nausea in patients hospitalized with cancer." Cancer Nursing, Vol. 23, No. 3, 2000, pp. 237-43.
Google Scholar Crossref - Ernst, Edzard. "Is reflexology an effective intervention? A systematic review of randomised controlled trials." Medical Journal of Australia, Vol. 191, No. 5, 2009, pp. 263-66.
Google Scholar Crossref - Elshamy, K. A. R. I. M. A., and E. M. A. N. Elsafety. "Effect of nursing interventions using foot reflexology on blood pressure and quality of life of hypertensive patients at Mansoura University hospitals: Preliminary results." Medical Journal of Cairo University, Vol. 79, No. 2, 2011, pp. 193-02.
Google Scholar - Embong, Nurul H., et al. "Revisiting reflexology: Concept, evidence, current practice, and practitioner training." Journal of traditional and complementary medicine, Vol. 5, No. 4, 2015, pp. 197-06.
Google Scholar Crossref - Embong, Nurul Haswani, et al. "Perspectives on reflexology: a qualitative approach." Journal of traditional and complementary medicine, Vol. 7, No. 3, 2017, pp. 327-31.
Google Scholar Crossref - Khalili, Arash, et al. "The effect of foot reflexology on physiological parameters." International Journal of Medical Research & Health Sciences, Vol. 5, No. 9, 2016, pp. 50-54.
Google Scholar - Elsayed, Amira E., Nahed A. Kandeel, and W. W. El-Aziz. "The Effect of Foot Reflexology on Physiological Indicators and Mechanical Ventilation Weaning Time among Open-Heart Surgery Patients." American Journal of Nursing, Vol. 7, No. 4, 2019, pp. 412-19.
Google Scholar - Ramezanibadr, Farhad, et al. "The impacts of foot reflexology on anxiety among male candidates for coronary angiography: A three-group single-blind randomized clinical trial." Complementary Therapies in Clinical Practice, Vol. 32, 2018, pp. 200-04.
Google Scholar Crossref - Jane, Sui-Whi, et al. "Effects of massage on pain, mood status, relaxation, and sleep in Taiwanese patients with metastatic bone pain: a randomized clinical trial." Pain, Vol. 152, No. 10, 2011, pp. 2432-42.
Google Scholar Crossref - Kunz, Barbara, and Kevin Kunz. "Complete Reflexology for Life: The Definitive Illustrated Reference to Reflexology for All Ages—From Infants to Seniors". Dorling Kindersley Ltd, 2008.
Google Scholar - Rambod, Masoume, Nilofar Pasyar, and Mohammad Shamsadini. "The effect of foot reflexology on fatigue, pain, and sleep quality in lymphoma patients: a clinical trial." European Journal of Oncology Nursing, Vol. 43, 2019.
Google Scholar Crossref - Khaledifar, Ali, et al. "The effect of reflexotherapy and massage therapy on vital signs and stress before coronary angiography: An open-label clinical trial." Arya atherosclerosis, Vol. 13, No. 2, 2017, p. 50.
Google Scholar - Vardanjani, Mehdi M., et al. "A randomized-controlled trial examining the effects of reflexology on anxiety of patients undergoing coronary angiography." Nursing and midwifery studies, Vol. 2, No. 3, 2013, pp. 3-9.
Google Scholar Crossref - Shahsavari, Hooman, Marzieh E.E. Abad, and Mir S. Yekaninejad. "The effects of foot reflexology on anxiety and physiological parameters among candidates for bronchoscopy: A randomized controlled trial." European Journal of Integrative Medicine, Vol. 12, 2017, pp. 177-81.
Google Scholar Crossref - Sheikh, Sara, Fariba Yaghoubinia, and Ali Navidian. "Impact of foot reflexology massage on the patients’ physiological indicators without trauma with loss of consciousness in the intensive care unit." Indian Journal of Public Health Research & Development, Vol. 8, No. 2, 2017, pp. 201-06.
Google Scholar Crossref - Mansouri, Ali, et al. "Evaluation of the effect of foot reflexology massage on vital signs and anxiety after blood transfusions in children with thalassemia." Bali Medical Journal, Vol. 6, No. 3, 2017, pp. 623-29.
Google Scholar - Ghazavi, Akram, et al. "Evaluation of the effects of foot reflexology massage on vital signs and chemotherapy-induced anxiety in children with leukemia." Medical-Surgical Nursing Journal, Vol. 4, No. 4, 2016, pp 41-48.
Google Scholar - Rodrigues, J., and Larissa Sams. "Effectiveness of foot and hand massage on postoperative pain, anxiety and selected physiological parameters among postoperative open heart surgery patients in cardiothoracic intensive care units of selected hospitals of Mangaluru." International Journal of Applied Research, Vol. 4, No. 5, 2018, pp. 461-74.
Google Scholar - El-Refaye, G., et al. H. ''The blood pressure response to foot reflexology adjunct to transcendental meditation training on postmenopausal hypertension.'' Physical Therapy and Rehabilitation, Vol. 4, No. 4, 2017, pp. 1-8.
Crossref - Ebadi, Abbas, et al. "The effect of foot reflexology on physiologic parameters and mechanical ventilation weaning time in patients undergoing open-heart surgery: A clinical trial study." Complementary therapies in clinical practice, Vol. 21, No. 3, 2015, pp. 188-92.
Google Scholar Crossref - Rollinson, Kirsty, et al. "The acute (immediate) effects of reflexology on arterial compliance in healthy volunteers: A randomised study." Complementary therapies in clinical practice, Vol. 22, 2016, pp. 16-20.
Google Scholar Crossref - Rahmani, Zohre, et al. "Effect of hand reflexology on anxiety and physiological variables among patients hospitalized in the cardiac care unit: a randomized placebo controlled clinical trial." Journal of Nursing Education and Practice, Vol. 8, No. 4, 2017, pp. 35-42.
Google Scholar Crossref - Moghimi-Hanjani, Soheila, Z. Mehdizadeh-Tourzani, and Mahnaz Shoghi. "The effect of foot reflexology on anxiety, pain, and outcomes of the labor in primigravida women." Acta Medica Iranica, Vol. 53, No. 8, 2015, pp. 507-11.
Google Scholar - Dehghanmehr, Sadegh, et al. "The impact of foot reflexology massage on anxiety caused by blood transfusion in children with thalassemia." International Journal of Pharmaceutical Sciences and Research, Vol. 9, No. 5, 2018, pp. 2053-57.
Google Scholar - Bagheri-Nesami, Masoumeh, et al. "The effects of foot reflexology massage on anxiety in patients following coronary artery bypass graft surgery: a randomized controlled trial." Complementary therapies in clinical practice, Vol. 20, No. 1, 2014, pp. 42-47.
Google Scholar Crossref - Rahmani Vasokolaei, Z., et al. "Comparison of the effects of hand reflexology versus acupressure on anxiety and vital signs in female patients with coronary artery diseases." Healthcare. Vol. 7. No. 1, 2019.
Google Scholar Crossref